Ocular diseases first described by Japanese doctors (eds by N.ohba)
Oguchi's disease
Oguchi's disease, first described by Chuta Oguchi in 1907. is a rare autosomal recessive trait characterized by congenital stationary night blindness and an unique morphological and functional feature of the retina. Patients have nonprogressive night blindness since young childhood with normal day vision, and they often claim improvement of light sensitivities when they remain long in dark conditions; dark-adaptation study may demonstrate that highly elevated rod thresholds decrease for initial many hours and eventually result in a recovery to the normal or nearly normal level. The eyeground in Oguchi's disease is so characteristic that it has a diffuse or patchy, silver-gray or golden yellow metallic sheen from the optic disk to the periphery and the retinal vessels stand out in relief against the radiant background. A prolonged period of dark adaptation, at least three hours, leads to disappearance of the unusual discoloration disappears and the fundus may assume its normal reddish appearance; the event is called Mizuo-Nakamura phenomenon. Oguchi's disease is also unique in the electroretinographic responses in the light- and dark-adapted condition. Recent identification of the arrestin gene mutation in patients with Oguchi's disease may account for the characteristic fundus and functional abnormality. The photographs illustrate unique fundus appearance in the ordinary light condition and in the prolonged dark adaptation condition (Mizuo-Nakamura phenomenon) in two patients with Oguchi's disease, one patient in Tokyo and the other in Kagoshima.

Oguchi Chuta (1975-1945)
Japanese ophthalmologist, Professor Emeritus of Nagoya University. He graduated from a private medical school in Tokyo (Saisei Gakusha) and passed the National Examination for Medical Practice in 1891. He learned Ophthalmology under Dr. SUDA Tetsuzo, and then at the Postgraduate Course of Tokyo University under Prof. KOMOTO Jujiro. He became an Army Surgeon and worked at many hospitals in Japan and in Taiwan. In 1907 at the Army Hospital in Tokyo, he examined a soldier who complained of night blindness: the patient was suspected of malingering. Dr. Oguchi found a peculiar fundus color with golden and mottled appearance and dark retinal vessels. He also found that the parents of this patient were cousins (J. Jpn. Ophthalmol. Soc. 11: 123, 1907). He further added similar cases in 1910, and concluded that this is a distinct clinical entity with congenital hemeralopia with recessive inheritance (Ueber die eigenartige Hemeralopie mit diffuse weissgraulicher Verfaerbung des Augenhintergrundes, v Graefe Arch Ophthalmol. 81: 109,1912). Prof. J. KOMOTO named it as Oguchi's Disease. He studied at University of Heidelberg and at the University of Munich in 1912-1914. After his homecoming, he received the degree Doctor of Medical Sciences from Tokyo University in 1916. He was appointed the Professor and Chairman of the Department of Ophthalmology of Nagoya University in 1922 and worked until retirement in 1939: he was entitled the Professor Emeritus of the University. He delivered a special lecture at the 40th Congress of the Japanese Ophthalmological Society in 1936, and served as the 41st Congress President of the Society in 1937. He also served as a Member of the International Council of Ophthalmology 1929-1937. He was granted the Japan Academy of Science Award in 1933 for his work on Oguchi's disease. In recognition of his service, the Government conferred on him the Second Order of the Sacred Treasures.(Cited from International Biography and Bibliography of Ophthalmologists and Vision Scientists,IBBO. Jean-Paul Wayenborgh, Saiichi Mishima and C. Richard Keeler. J.-P. Wayenborgh, Belgium, 2002)
ü@
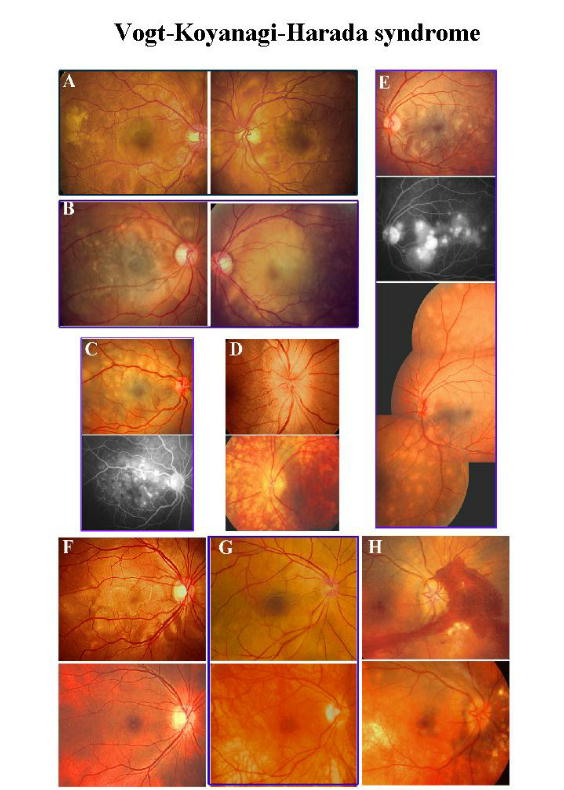
Harada's disease
Vogt-Koyanagi-Harada syndrome, also called Harada's disease, is an acute inflammatory, immune-mediated disorder that typically affects middle-aged adults and involves melanocyte-containing organs such as the skin, ear, meninges, and eye.Acute exudative panuveitis occurs in both eyes and causes ocular irritations and visual loss. Upper photographs show acute the phase of the disease featuring neurosensory retinal detachments associated with multiple loci of aggressive choroidal exudations. Some patients may present with predominant optic disk swelling. A large dose of systemic corticosteroids is a rewarding treatment for a rapid resolution of exudative lesions. Lower photographs illustrate a common outcome of Harada's disease, "sun-set glow" albinotic fundus, often accompanied by cutaneous pigment deficiencies. The disease is essentially benign when managed properly, but it may sometimes become smoldering and result in development of retinal and choroidal neovascularization, severe chorioretinal atrophy, and secondary glaucoma.
Einosuke Harada (1892-1946) Japanese ophthalmologists. He graduated from Tokyo University in 1917 and studied Ophthalmology under Prof. J. Komoto and Prof. S. Ishihara. In 1922, he discovered a rare case of acute uveitis with bilateral retinal detachment. He compiled similar cases and established a new clinical entity, which is now named "Harada disease". Later it was found that this disease together with the diseases described by A. Vogt and Y. Koyanagi is an expression of the same disease entity, i.e., Vogt-Koyanagi-Harada disease. Dr. Harada carried out research at the Department of Pharmacology and was granted the degree, Doctor of Medical Science for studies of ocular pharmacology. In 1930 he started to practice in the city of Nagasaki; his hospital was destroyed by the atomic bomb. Although he survived the bomb, he died before he could restart practice. (Cited from International Biography and Bibliography of Ophthalmologists and Vision Scientists,IBBO. Jean-Paul Wayenborgh, Saiichi Mishima and C. Richard Keeler. J.-P. Wayenborgh, Belgium, 2002)
Einosuke Harada was born Hondo-cho which is located in one of Amakusa islands middle of Kyushu, southwestern Japan. He attended the Fifth National High School at Kumamoto (now Kumamoto University) to finish premedical course and graduated in 1917 from Tokyo Imperial University Medical School. During a medical student he was granted tuition fee and expenses from the Japanese government and after graduation on contract he worked for the national army hospital for two years.
Dr. Harada began a carrier of ophthalmology at Tokyo University Hospital on June. Harada decided to specialized ophthalmology, Dr. Shinobu Ishihara had taken a chair of ophthalmology of the University, the second chairman succeeding the first [Professor of Ophthalmology, Jujiro Komoto, and the Department had then a mood of refreshment and reactivation. Five months after starting ophthalmology residency, Dr. Harada encountered a remarkable patient. According to his note,
The patient is a 47-years-old man. He presented with bilateral, acute visual loss, with vitreous opacities, hyperemic optic disks, retinal edematous opacities, and thereafter the retinal edema showed a gradual increase. Hospital day 21, a mild nonrhegmatogenous exudative retinal detachment was noted in the inferior quadrants of both eyes. Then, reported to Professor Ishihara, he suspected of bilateral generalized choroiditis or diffuse uveal disorder, but there was were neither keratic precipitates nor changes of the iris. On that day, the former Professor Komoto, retiring nearby, came incidentally to the office, and on consultation he emphasized acute, bilateral exudative choroiditis, and after returning home Professor Komoto told me on a telephone that the disease seems rare and recommend to study in details.
He reported the case on December 17 for a meeting of Tokyo Ophthalmogical Association and published a case report the next year (Japanese Review of Clinical Ophthalmology (Ganka Rinsho Iho). In the subsequent two years, Dr. Harada experienced successively and published four similar cases in 1939 in the same journal and in 1940 in Acta Ophthalmologicae Societasis Japonicae (Nippon Ganka Gakkai Zasshi). As such, it is remarkable that Dr. Harada found and recognized the first case in the first year of residency. As a young he must have a condition of enrichness for a discovery of a new disease entity, meticulous attentive attitude, ardent vigilance, hard-working spirit, and luck of having interesting cases. Moreover, the time was that Dr. Shinobu Ishihara, a man of academic ophthalmology and well known for invention of the Ishihara pseudoisochromatic plates for detection of congenital color blindness, was appointed as a chairman of the Department and had started to build a new academic institution.
A word should be added about the relation to Dr. Yoshizo Koyanagi, Vogt-Koyanagi Harada syndrome. Dr. Harada published original cases in 1923. Six years later (1929) Dr. Koyanagi reported four new cases. Dr. Koyanagi was 12 years senior to Dr. Harada and he was then professor and chairman of Department of Ophthalmology of Tohoku Imperial University at Sendai (northern Japan), another influential institution of the country. Dr. Koyanagi published his cases in German in Klinische Monatsblaetter Augeneheilkunde as a 18-page big paper which contained then unusual colored figures. In contrast, Dr. Harada was then a young trainee and his publications were all written in Japanese except for a paper with a short German abstract in 1933. However, it is noticeable that the reported cases were outnumbered by Dr. Harada, and it seems natural that in Japan the disease was called Harada' disease (Harada byo). Soon after reports by Drs. Harada and Koyanagi many cases of the entity were described first in Japan, and then the disease had been known abroad.
The worldwide literature indicates that of 60 papers reporting the disease, 55 named Vogt-Koyanagi-Harada syndrome, and 5 Harada disease, thus predominated by Vogt Koyanagi-Harada (VKH) syndrome. In my experience, I often hear 'Harada disease' in the United States, which may be short and easy to pronounce in daily communication. I prefer Harada disease at least when the disease is primarily confined to the fundus.
The designation Harada disease received some controversies when the disease was reported. Dr. Harada said, "... If asked to name, the disease was called Komoto-Ishihara Harada disease in honor of my professors since I was instructed much by my mentors, and as I could study many cases during three years during my residency in Department of Ophthalmology Tokyo University the disease is otherwise designated memory of the institution. .... I will be happy myself if a new entity is recognized as acute, diffuse exudative choroiditis, and I think that the designation Harada disease does not tell what site of the disease." Dr. Harada was a modest man and enjoyed haiku writing, leaving many beautiful pieces of original haiku.
Dr. Harada published some 10 papers on the disease, all published in clinical ophthalmology journals, and the papers were written in a simple and easily understandable description. Dr. Harada was a lifelong zen trainer. Professor Ishihara recommended young doctors to take zazen to train personality to attend several times a month training field, and he was probably only one who had a master of zen among Ishihara's students. One man asked Dr. Harada 'It is surprising why the disease remained unrecognized before you first described', and he answered 'We are usually concerned seriously with the past documentations and the literature. It seems important, however, that we are always aware of and attentive things before us and have to observe as they are, and then we could naturally discover new facts.' (Translated from S Fujino: Discovery of Harada disease and Dr. Harada Einosuke. J Jpn Ophthalmol Soc, Special Issue 1996)
ü@